



Why is the monkeypox epidemic improving?
Insights from two new technical reports

U.S. CDC is back with another monthly monkeypox technical report. You can read my reads of previous reports here and here.
Since the August edition, the U.S. monkeypox epidemic has taken a turn for the better. Case counts have been declining steadily and the feared expansion into populations other than men who have sex with men (MSM) has not happened. Over 95% of cases in the U.S. are still in men, and most cases still report a history of MSM sexual contact. In New York City, one of the earliest-hit places in the United States, the average daily case count is now in the single digits. In California, it’s sub-30, the lowest it has been since July.

To what do we owe this success?
First, a brief rewind. On Wednesday the agency released a preliminary analysis that shows a substantial reduction in case rates in people who had received at least one dose of Jynneos, the monkeypox vaccine. Because of the way the study was conducted, the analysis cannot determine that vaccination is responsible for the lower incidence—there could be differences in people who chose to receive the vaccine that may also influence whether they were exposed to the virus. For example, people who got vaccinated may have been more likely to change their sexual behaviors. We just don’t know.
A reader could draw a dotted line between the vaccine analysis and control of the epidemic. Perhaps the vaccine works very well, and so many people are protected that the virus is not circulating efficiently. Well, an analysis in the technical report suggests that there is more to the story. The authors say:
Our estimates for rates of outbreak growth suggest the reproductive number began slowing at a time when vaccine coverage was still very low. Specifically, the mean Rt estimate crossed 1 on approximately July 31…[when] vaccine-induced immunity by late July was approximately 1.3%
In other words, the epidemic began shrinking when less than 2% of the people at highest risk were vaccinated. That level of coverage is not enough to provide meaningful protection at the population level. Therefore, it’s likely behavior change (and potentially case-based interventions like contact tracing) that bent the curve, not exclusively vaccination.
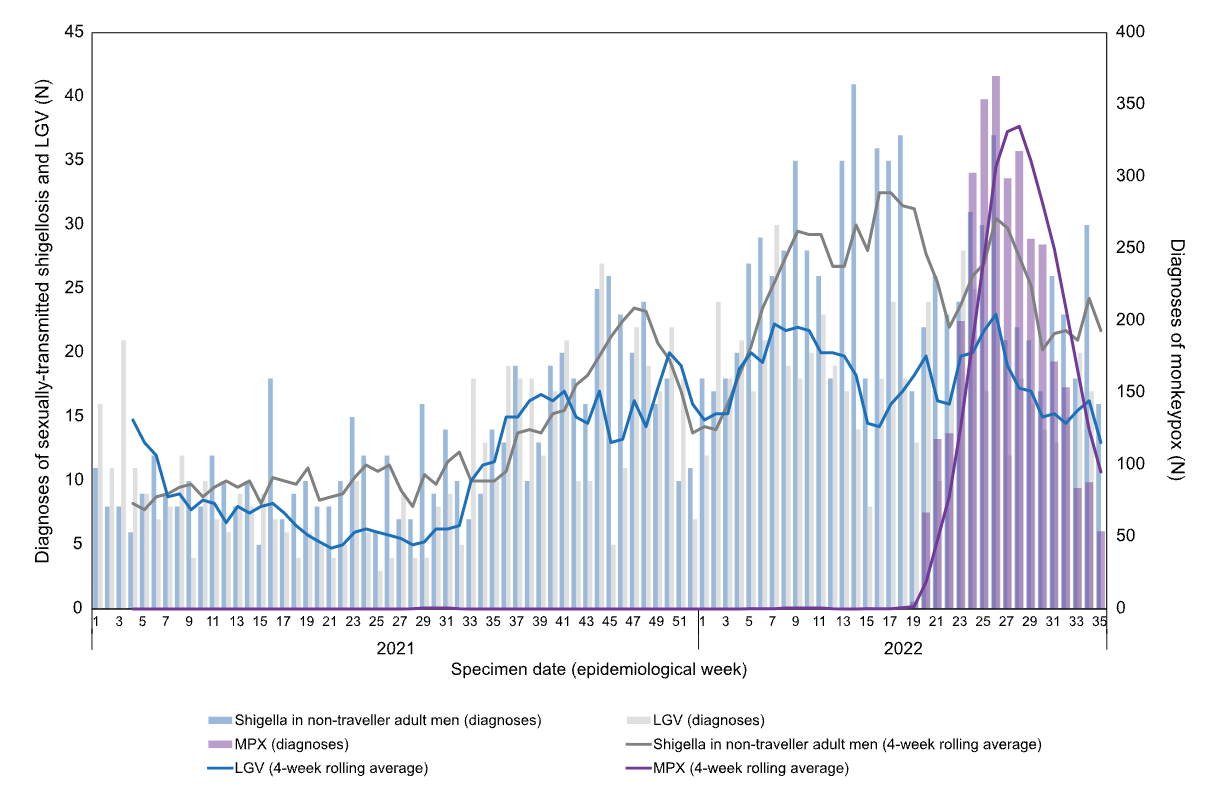
Additional evidence comes from the latest technical report out of the UK Health Security Agency. Epidemiologists there took a clever approach to get at the question of whether the recent downturn is attributable to behavior. They looked at the number of new diagnoses of Shigella and lymphogranuloma venereum (LGV), both infections spread through close contact that disproportionately affect MSM populations. If improvement in the monkeypox epidemic was attributable to vaccination, transmission of those diseases would be unaffected. Results show a modest decrease in the number of new Shigella and LGV cases, suggesting that in fact behavior is playing a role.
Conversely, this does not mean the vaccine does not work. In fact, one modeling study reported in the UKHSA document suggests that as much as half of improvement there is attributable to vaccination. But behavior is likely playing an important role in recent improvements in the epidemic trajectory, and so we could see a rebound of monkeypox cases if behavior changes again.
The U.S. technical report shares that view: “…we assess daily cases in the United States will most likely continue to decline or plateau over the next two to four weeks. We have moderate confidence in this assessment but note the possibility that incidence could increase again.”
For now, the outbreak is improving markedly and I hope to see that continue all the way through to elimination.
I'm really getting a ton out of your coverage of monkeypox I haven't read elsewhere. Thanks so much for your continued thoughtful analysis :)
It's helpful to see you compare Shigella and LGV to monkeypox to see how behavior change is influencing case rates. It's a good reminder that bread and butter public health works!