



This week in outbreaks
Ebola, monkeypox and influenza like illness

As foretold, my household (and seemingly everyone we know) has been taken down this week by flu-like illness, so today’s newsletter is abbreviated. I will be back next week with an interview with an expert on how our immune systems develop to discuss the latest on the hygiene hypothesis. Until then, here is a roundup of things I am following.
Ebola
The Ebola outbreak in Uganda remains concerning. At least 63 confirmed and probable cases have been reported, including 29 deaths. Sadly, ten of those cases are in healthcare workers and four have died. The outbreak is caused by Sudan ebolavirus, for which the existing Ebola vaccines and therapeutics are not expected to work. Responders are using contact tracing, isolation, quarantine, and community education and engagement to slow transmission.
U.S. CDC recently announced that all travelers who have recently been in Uganda must enter through one of five airports, where they will undergo temperature and symptom screening for the virus. This has become standard practice across recent outbreaks, though it’s not shown to be especially effective at identifying infections.
Monkeypox
The monkeypox outbreak continues to slow in the United States. As of October 5, the average number of daily cases was just 68, the lowest since June (476 cases in the last week). The number of people tested and the number of people receiving first doses of the vaccine has also continued to decline. Similar trends are seen in Europe, where the weekly number of cases is now below 250. In the United Kingdom, there were only 19 cases reported in the last week.
However, according to Africa CDC there are a number of cases in lower resource settings, including West and North Darfur, Sudan. There were also 553 new cases reported in the Democratic Republic of Congo, bringing the total there to nearly 3,500. As the WHO’s Director-General reminded us when he declared the monkeypox outbreak a Public Health Emergency of International Concern, the global public health community must “implement a coordinated response to stop transmission and protect vulnerable groups.”
Influenza and other respiratory illnesses
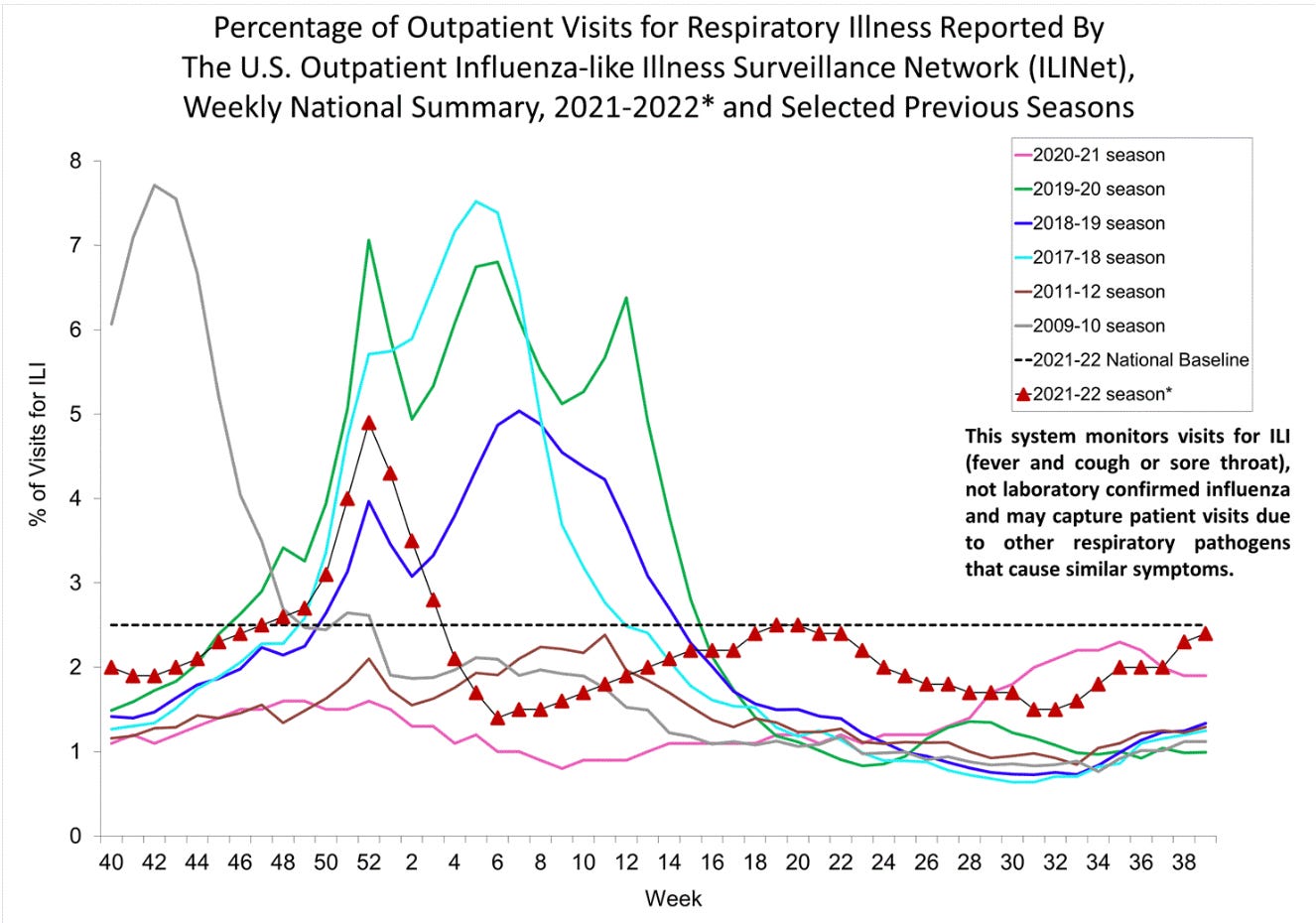
This week the U.S. continued its journey into flu season About 2.5% of the 1,021 specimens tested came back positive, an increase over last week. The percent of outpatient visits for influenza like illness (ILI), a measure that encompasses both influenza and related flu-like illnesses, also crept up this week. Texas, Georgia, and the District of Columbia are reporting high levels of ILI. Nationally, as in previous weeks, kids ages 0-4 are heavily affected.
Many state and local jurisdictions begin publishing their influenza like illness surveillance reports in October, so more sources of data will be coming online in the near future. Forecasting of influenza hospitalizations will also resume this fall.
A thought experiment: In my experience, some states didn't exactly publish accurate/truthful data during COVID. What are the chances they'll not be forthcoming about flu now because they don't want some word to get out about their levels of infection? Or is my paranoia showing?